Forming long lasting relationships by managing rising healthcare costs through high quality

Addressing Pharmacy Benefit Management Misalignment
High prescription drug costs continue to bankrupt families, put financial strain on businesses, and drag down the US economy and pharmacy benefit management plays a significant behind-the-scenes role. To arm employers and other plan sponsors with a blueprint to...

Protecting Employee Health in the Workplace
This 2-page resource helps clear up confusion about respiratory virus prevention recommendations to help protect American families and businesses from another disruptive surge. Want to learn more about Proven Workplace Strategies to Improve Vaccination Rates and...

New Directions to Better Manage High-Cost Claims
High-cost claims have become the single fastest growing healthcare cost for employers in the last decade; a significant threat to employer-sponsored healthcare benefits. This Action Brief includes steps employers and other plan sponsors can take to mitigate high-cost...

The 40% “Cadillac Tax” Has Been Repealed
Washington, D.C. – Today, the Alliance to Fight the 40|Don’t Tax My Health Care, a broad-based coalition committed to repealing the 40% tax on employer-provided health benefits, today applauded the president for signing in to law H.R. 1865, the end-of-year...

How Health Insurance Costs Have Changed Throughout the Years
Healthcare costs can be quite expensive. For some people, a serious or prolonged illness could be the impetus for financial devastation. Even a trip to the emergency room for a minor injury could result in major expenses. Fortunately, health insurance coverage can...

What Employees Look For In Their Company Health Plan
If you have to find a health plan for your company, you know just how difficult this can be. You want to get a plan that meets everyone’s needs, but you also don’t want to have to pay an exorbitant amount for it. Fortunately, you can narrow down your search by knowing...

CBD oil as medicine: The promise and the risks
Metro Atlanta resident Becky Ferguson says she started using non-addictive cannabis oil because she hoped it would ease her chronic pain.The result was not quite what she expected.“It might have helped a little bit [with the pain], but I am getting a tremendous...
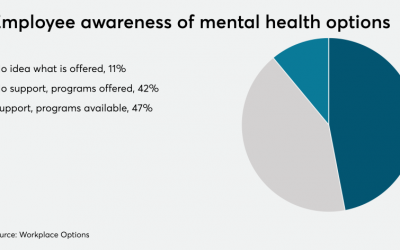
National Alliance of Healthcare Purchaser Coalitions launches five-year plan on mental health
WASHINGTON — The National Alliance of Healthcare Purchaser Coalitions introduced a five-year plan on Monday to push employers and health systems to address mental health and substance abuse issues for employees. Michael Thompson, president and CEO of the National...

How to Get Affordable Health Insurance For Businesses
Finding affordable health insurance isn't just a problem for individuals anymore. Affordable health insurance for businesses is also a difficult thing to obtain for many companies. Securing insurance for your business is one of the most intimidating tasks when running...

Second vaping-related death reported in Georgia
ATLANTA, Ga. (WTOC) - The Georgia Department of Public Health is reporting the state’s second death from a vaping-related illness.Health officials say the patient had a history of nicotine vaping, but the case is still being investigated to determine if other...